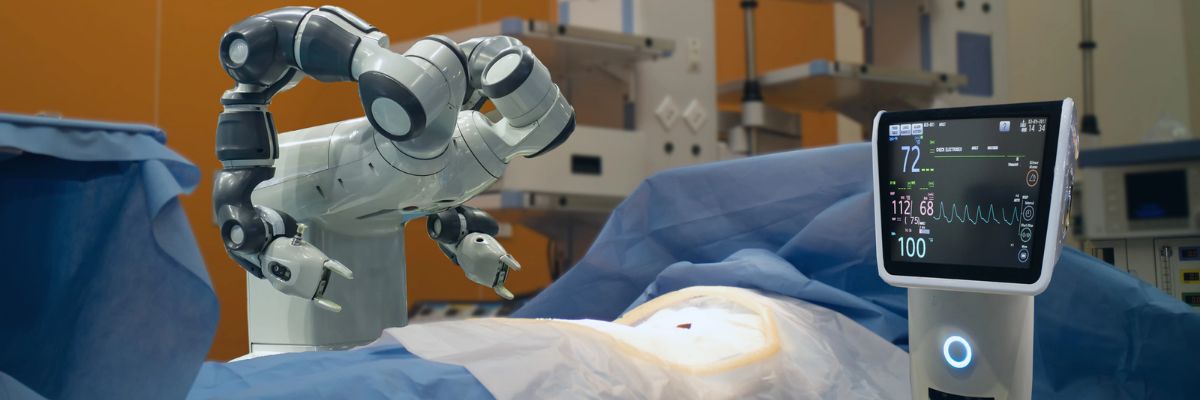
What are the steps involved during our “tailored” robotic prostatectomy?
Posterior dissection of seminal vesicles and prostate
The seminal vesicles are cystic structures attached to the prostate and function in storing and adding nutrients to the semen. The seminal vesicles are always removed with the prostate during surgery. A posterior approach enables energy-free and traction-free dissection of the nerve bundles that run along the sides and tips of the seminal vesicles.
The posterior approach also allows for perfect visualization of large or asymmetric seminal vesicles, situations which could be very complicated in an anterior approach. Additionally, this approach will enable us to bypass a large median lobe (a protrusion of the prostate into the bladder) without compromising visualization.
Developing the space of Retzius and anterior prostate dissection with sparing of the Endopelvic Fascia
This step drops the bladder and the prostate from the abdominal wall. It allows the surgeon direct visualization of the anterior prostate and the dorsal vascular complex. By sparing the Endopelvic fascia, an Intra-fascial dissection is more likely to be successful. See neurovascular bundle dissection below for more details.
Division of the prostate from the bladder by the bladder-neck sparing technique to preserve the internal sphincter mechanism
Two layers of bladder muscle fuse together the bladder and prostate in addition to fatty tissue. This area includes the internal urinary sphincter, which is composed of muscle fibers that play a role in the subconscious control of urinary function. In most patients, preservation of the bladder neck sphincter mechanism can result in early urinary continence. Proper preservation can also reduce the risk of strictures or scars at the bladder neck, commonly referred to as bladder neck contractures.
When the bladder neck is not spared, the subsequent large opening may necessitate a time-consuming reconstruction to narrow the opening. Larger openings also require a longer suture line and, therefore, may be more susceptible to leakage of urine from the anastomosis. Given all these factors and assuming there are no biopsy features putting the patient at risk for bladder neck involvement or the presence of a large median lobe, we always strive to preserve the bladder neck.
Dissection of the lateral prostatic fascia and sparing of the neurovascular bundles (NVB)
The nerve bundles carry neural information and blood flow into the deep pelvis. These structures are critical for both erections and urinary control after surgery. Multiple studies to date have shown a direct relationship between the degree of nerve sparing and post-operative potency and urinary control.
Contrary to what most patients believe, nerve sparing is not an all-or-nothing concept. Depending on the extent of the cancer, the nerve dissection can be individually tailored to the patient and their cancer.
Many factors come into the decision but include the risk of extracapsular extension based on pre-operative nomograms/risk-tables (link to separate section/post), the results of pre-operative T3 MRI of the prostate (link so section), the findings of a rectal exam under anesthesia, intra-operative findings and the ease of “peeling” the bundles away from the prostate.
The degree of precision and dexterity that is needed to dissect the nerve bundles away from the prostate is similar to what is required to “peel” the skin off of a tabletop grape (link to video).
Our goal is to remove all prostate and cancerous tissue clearly, but as important as a goal is to leave all non-prostate tissue as it was before the surgery. Many times, surgeons use the terms extrafascial, interfascial, and intrafascial to describe different techniques to dissect the prostate and the nerve bundles.
Extrafascial: This is also known as non-nerve sparing or wide-excision dissection. When there is either high suspicion that the tumor has penetrated the capsule wall deep into the extracapsular fatty tissue or is involving the nerve bundle itself, this may require us to resect the nerve bundle altogether with the prostate.
Typically, a preoperative MRI can determine the extent of involvement. In this type of dissection, the endopelvic fascia is incised deep near the levator ani muscles to carry out this type of dissection. In patients who are not interested in nerve preservation due to baseline erectile dysfunction, a wide excision may not be critical.
However, even in patients with clear evidence of extracapsular involvement, we may be able to do a graded dissection and spare some of the neurovascular bundle on the side affected with cancer in hopes of maximizing post-surgical potency. We use intra-operative frozen sections whereby we send tissue at the edge of the dissection to get a preliminary assessment of any tumor at the margin and subsequently guide our dissection based on those results.
We are also currently working on a novel technology that will enable the real-time identification of prostate tumors using fluorescent dyes targeting the cancer and near-infrared imaging, similar to what we have pioneered with kidney cancer surgery (link to Firefly). Although we are currently evaluating this technology in an animal model, we hope to apply this to clinical use soon and recruit patients into a clinical trial.
Interfascial dissection: The endopelvic fascia is incised, and the neurovascular bundles are spared posterolaterally to take some of the tissue around the prostate (periprostatic fascia) with the specimen. The component of nerves and vessels that can sometimes be found on the anterior aspect of the prostate are therefore not spared. As noted above, the clinical extent of the tumor has an impact of whether or not we decide to do this type of graded dissection.
Intrafascial dissection: This is the most delicate and precise type of dissection. Think of this as a custom-made, very “fitted” type of dissection. In this type of dissection, the endoplevic fascia, the neurovascular bundles, the periprostatic fascia, and Denonvillier’s fascia are all spared and left intact. The plane of dissection is directly guided on top of the prostate capsule. By preserving all these structures, we maximize the patient’s chance of regaining erectile function and urinary control after surgery.
Control of dorsal vascular complex (DVC)
As its name implies, the DVC contains an array of both veins and arteries that carry and drain blood from the penis. Due to the large amount of blood flowing in this structure, inadvertent injury can result in a significant amount of bleeding. The higher amount of blood loss associated historically with open prostatectomy techniques was related directly to this point of the procedure.
Fortunately, with the utilization of CO2 gas for laparoscopic and robotic surgery, venous bleeding from the DVC is no longer a major issue, as the gas can provide passive pressure and prevent oozing from this area. Two methods are used to control the DVC: either suture ligation or endoscopic stapling.
One of our preferred methods of control is to use an endoscopic stapler. As we have previously published, endoscopic stapling allows for a consistent, efficient, and reliable method for getting control without risking a positive margin at the apex of the prostate.
Preparation of Apical Urethra – preserve length and muscle fibers
Prostates come in all sizes and shapes. Some are smaller, some are bigger. Most of the variation in shape is usually seen at the apex. The apical prostate surrounds the urethra near the external sphincter complex. The goal at this point of the operation is to achieve a long and thick urethral stump that will subsequently be reconnected to the bladder neck.
There is a fine line between dissecting too deeply (the levator muscles and the external sphincter complex can be inadvertently damaged) and too shallowly (risk leaving prostate tissue behind).
Posterior Reconstruction
Also known as a Male sling, Rocco reconstruction, or Rhabdosphincter reapproximation. This technique provides posterior support for the sphincter complex, similar to a hammock, and prevents the urethra from slipping further down into the pelvis during activity, which may lead to leakage, such as during coughing, sneezing, or laughing.
The reconstruction also brings the bladder down into a supported position and therefore removes any tension on the completed urethra-bladder anastomosis. Most experts agree that this type of reconstruction leads to shorter recovery times for urinary control.
Urethrovesical anastomosis
The goal at this point of the procedure is to create a watertight and tension-free connection between the urethra and the prostate. One of the most significant advancements to our practice has been the ability to utilize a barbed suture (V-Loc, Covidien) that maintains the reapproximated ends without allowing any gaps between the tissue edges. As a result, for years now, we have avoided using any post-operative drains unless we are dealing with a very large bladder neck or a reconstructed bladder neck.
Pelvic Lymph Node dissection: Removal of pelvic lymph nodes – extended dissection for patients at greater risk of involvement based on biopsy features, clinical exam and PSA
Even though pre-operative CT or MRI may not show evidence of regional lymph node involvement, the accuracy of these imaging tests is only around 80%. The decision to identify and remove the lymph nodes that drain the prostate during prostatectomy is made on an individual basis. We calculate the risk of lymph node involvement based on widely available nomograms and risk calculators such as D’Amico criteria, Partin Tables, CAPRA score, or MSKCC calculator.
Low-risk patients (for example, those with PSA <10, Gleason 6, or clinical T1c) do not benefit from a lymph node dissection. Intermediate-risk patients and High-risk patients, on the other hand, may benefit from a lymphadenectomy. It is believed that an extended lymph node dissection (in both lymph node negative and positive patients) may lead to the removal of undetected micrometastases, and therefore improve the survival of patients undergoing prostatectomy.
There is a growing body of evidence suggesting that the greater the number of lymph nodes removed, the more beneficial. However, no uniform consensus exists regarding the limits of the boundary of the dissection or the minimum number of lymph nodes that should be removed. Historically, the detection of suspicious lymph nodes at the time of radical prostatectomy led many surgeons to abandon the operation with the belief that regional lymph node involvement was a sign of widespread metastatic disease and therefore associated with poor prognosis.
Patients would subsequently be referred for treatment with hormones and/or radiotherapy. However, there have been several recent studies showing very reasonable cancer-specific survival rates even in patients with lymph node-positive disease at the time of radical prostatectomy. A recent publication from the European Journal of Urology analyzed the Munich cancer registry and found that patients with lymph node-positive disease who did not have their operation aborted on average had a 20% improvement in survival compared to those who had their operation aborted.
Dr Josephson has a special place in my heart. He is a truly wonderful human being.
Etai A.
We’ve had a wonderful experience with Dr. Josephson. He is knowledgeable, kind and patient. I wish all my doctors were like him.
TIFFANY S.
Dr Josephson has a magic hand. after protate surgery usually most of the patients get leaks but mine was perfect. He is very intelligent, helpful, patient, and polite. I recommend him to all my friends and family
SHAWN M.
Dr Justin Houman has made a positive impact on my health. At first I was nervous about seeing a Urologist but he made me feel comfortable to open up and solve my problems. Highly recommend him. Five Stars ⭐️
Baguette M.
Justin is a very caring doctor who always goes out of his way to address my needs.
Alec P.
Very kind and professional Doctor. Caring and experienced staff. Lucky to have found Dr. Houman and I highly recommend him to anyone looking for a urologist.
Dreamland D.
I have been suffering from Testicular pain for the past 3.2 years, and it has been a challenging journey. If I do certain activities like long walks, lifting weights and sex triggers or worsen my testicular pain. The pain was intense enough to significantly impact my daily activities. Pain forces me to rest for 1 to 2 days and applying the Ice packs frequently.
I finally met Dr. Justin Houman, who has truly been my life saver. I recently underwent Microsurgical Spermatic Cord Denervation and Varicocelectomies Surgery with Dr. Justice Houman and I noticed a significant reduction in my chronic testicular pain, which has greatly improved my quality of life. I have gradually resumed activities like long walks, lifting weights, sexual activity and I am experiencing only very minimal testicular pain, which doesn’t affect my daily activities.
I would highly recommend Dr. Justice Houman to anyone suffering from chronic testicular pain, he is a true expert in men’s andrology.
Dr. Houman is truly a life saver for me, Thank you very much Dr. Houman!
Kishore C.
Dr.Josephson was an Answer to many prayers! I recently had surgery in Bakersfield
with urologist who is past his prime.
I couldn't get help after my TURP surgery.
For 3 months (90 days) I was in great discomfort, unable to urinate without extreme pain. 40 times a day,wanting to cry !
My Bakersfield urologist said there was NOTHING he could do to help me. A friend sent me to Dr. Josephine. I prayed for a miracle and Dr. Josephson kindly obliged.
No further surgery was needed! Dr.Josephson took the "time" to examine me and found the issue immediately and I left his office as happy a child !!
Thank you,Dr.Josephson, words cannot express my gratitude enough!! You helped me greatly in my time of need!
You were kind and gentle and made me feel cared for. Thank you,May God Bless You !!
JSM
John M.
I had a wonderful experience with Dr. Kuhlmann and her team. Her bedside manner was fantastic and put me at ease throughout my visits. She was responsive to my questions and fully explained my treatment plan. My quality of life has significantly improved and I am so thankful to have found a physician I can trust. Would 100% recommend.
Jacqueline R.
Dr . Josephson is hands -down the absolute best any patient or family could ask for in a doctor .
His staff is on point they run like a machine. The experience has been exceptional. His care knowledge understanding and follow up is on point and he truly is the best urologist you can find. highly recommend it .
Sarineh Y.
Very pleasant, helpful, and very knowledgeable doesn’t do any test, which is not necessary like most of the other Urologist do give you a clear opinion of your health and give you good advice I strongly recommend him I do wish him all the best in his career
David N.
A family member was struggling with testicular pain for years and had concerns about fertility. I am so grateful that we were referred to Dr. Houman. He is very thoughtful and knowledgeable and has great bedside manner. He diagnosed a varicocele and recommended microsurgical varicocelectomy and we are so happy with the results.
I highly recommend Dr. Houman.
Sophia L.
Dr Kuhlmann and her office were wonderful. She was attentive in answering my questions and made me feel heard. She was friendly, professional and helpful. I’d definitely go back if I had any future concerns!
Ruby W.
Amazing urologist. Go to expert for men’s health. I refer patients to him as often as possible!
Ilan K.
The best. I can’t say enough good things about the care i received and continue to receive from all the people at Tower urology especially Dr. Joesepson.
Robert H.
He saved my dad’s life. Thanks for everything you did. Can never repay you.
Amir Y.
How did a woman with a lifetime of recurrent bladder infections wind up with a urologist whose specialty is male fertility?
It happened like this...Dr. Houman was recommended to my husband when he began having the prostate problems that can devastate older men. Dr. Houman solved his urinary difficulties, and I'm convinced, kept him from the fate of a constant catheter.
Naturally, I jumped at the chance to be his patient, and have been, for the first time in my life, free for several months of any infections.
But the best part of being Dr. Houman's patient is this. When you are in trouble, he will keep in constant touch with you...he does not isolate himself behind a wall of nurses. Naturally, I recommend him highly,
Marilyn B.
Marilyn B.
Great doc you can trust. He's very up on all the new and modern modalities to help you and keep you healthy. Great choice and nice guy.
Dave R.
Fantastic! 3 surgeries! The guy is on top of his trade & switched on my full potentials for quality of life.
Many thanks to you Dr j.
❤️🎉🍾🎈🙏
Amir V.
Dr. Kuhlmann is AMAZING!! I saw her for perimenopause care and she explains everything clearly and got me started on a treatment plan right away. Highly recommend.
Heather J.
My experience with Dr. Houman has been nothing but positive. He takes the time to really listen and provide solutions. I came to him, very unsure and very unhappy, with a procedure done by another doctor several years earlier. After a couple of meetings Dr. Houman assured me that he could help me. And that’s exactly what happened. I'm very pleased with the results. His bedside manner and can-do attitude, his insight, enthusiasm and quick email responses were greatly appreciated. You can’t do better than Dr. Houman. I highly recommend him.
Russ W.
Dr. Kuhlmann was excellent at listening to my individual needs and exploring the best solutions possible.
C H.
10/10 would recommend!! Dr. Houman is the best!!
Arturo K.
Dr Houman gave me a new life with the Inflatable penile implant. In the past I tried viagra and injections but nothing compares to this procedure. As I am 79 I have the youth and lasting desire of love making as a 40 year old Mick Jagger! If you are reluctant .... Dr Houman is the best and most knowledgable!
Barry B.
Dr. Houman is a one of a kind doctor, truly. It's a scary thing to go see a urologist, and Dr. Houman made the experience comfortable, safe, and he instilled confidence in me as a patient. My fear and worries went from 100 to zero, and I am extremely happy to have found his office. Would recommend Dr. Houman to anyone!!
Ben M.
Excellent doctor! Was completely taken care of from start to finish
Jimmy L.
Thorough. Communicative. I would highly recommend Tower Urology and Dr. Josephson in particular.
Karl S.
Highly recommend Dr Houman he is amazing and saved my life
ROBERT D.
Highly skilled and compassionate, Dr. Houman provides excellent care suggestions.
S K.
Dr. Houman is excellent—professional, compassionate, and thorough. I felt well cared for and informed every step of the way. Highly recommend!
Mr. E.
Dr. Houman is knowledgeable, professional, and genuinely cares about patients. They made me feel comfortable and well-informed throughout the process. Highly recommend!
spicy G.
Best doctor in town!
Hannah N.
Best urologist in the game. It’s never too early to consult a doctor. Justin made me feel comfortable and work through different issues that were important to me to resolve. I met with a few doctors until I found Justin. He is top notch. Highly recommend
Ryan D.
Dr. Houman is a SUPERHERO.
He is everything you’d dream of in a doctor and more!
He takes care of my family with such kindness and expertise.
We are so grateful to this outstanding urologist - he is absolutely amazing!
Amanda M.
This is ari zoroaster dr. Houman is one of the best doctors I have ever had very professional and smart ...and super friendly that make you forget the pain of needles !!!!! Over all I am very pleased of knowing him and will keep going there.
martha F.
Dr. Houman is an outstanding urologist. He’s professional, knowledgeable, and kind. He really took the time to thoroughly answer all my questions. I would highly recommend Dr. Houman.
Ashley H.
Dr Houman is the urologist you’ve been looking for! He never shies away from a challenge and has taken excellent care of me over many hurdles! He’s dedicated to each patient, never in a rush and a talented surgeon!!
Thomas C.
Dr. Kuhlmann is a fantastic urologist — she really takes the time to listen and address your concerns. I couldn’t recommend her enough
Jeremiah D.
Dr. Kuhlmann is an excellent surgeon, physician, and clinician. She is very skilled, thorough, and attentive-she puts her patients first. I highly recommend her!
Tiffany P.
Dr. Kuhlmann is a brilliant doctor physician and excellent diagnostician. She truly listens to her patients’ concerns and uses up to date treatments. I fully trust I am receiving the best care from her!
Kayla L.
Dr. Houman was the most compassionate and caring doctor that we met in our 10 day stay at the hospital. He is a knowledgeable doctor that genuinely wants to help.
Joseph S.
Dr. Kuhlmann is extremely knowledgeable and a truly caring physician. She has a way of communicating confidence and expertise while also meeting each of her patients on their level. Very professional and goes the extra mile for everyone she cares for.
Samuel G.
Dr. Houman was amazing, don’t typically do reviews but he was extremely thoughtful and helpful. Highly recommend!
Michael S.
Best of the bests! Highly recommend Dr. Houman
Janet N.
Dr. Houman is the BEST! He literally saved my grandpa's life and he couldn't be more kind and thoughtful. If Dr.Houman is your doctor then you're in amazing hands!
Thank you Dr.Houman
Ella N.
Dr Kuhlmann is a fantastic physician. She is very caring and attentive. I appreciate her dedication.
Danielle B.
When my patient’s need a urologist, I go to Dr. Kuhlmann. She is my top choice for urologic care in the region.
Desmond Huynh, MD
Desmond H.
Excellent physician and great listener. Most physicians don’t take the time to understand or put themselves in their patient’s shoes. Dr. Kuhlmann is the opposite of that. Highly recommend.
Joleen H.
Dr. Paige Kuhlmann is a warm, caring, compassionate and smart doctor. She went out of her way to accommodate my mom and made her feel so comfortable. I give her a 10 out of 10!
Are outdated prostate cancer screening guidelines putting lives at risk? President Biden’s diagnosis sparks a national conversation on early detection.
Dr. David Josephson, Urologic Oncologist and Prostate specialist and Dr. Robert Princenthal, Medical Director of Radnet’s Prostate MRI program weigh […]
“Click here to grow your penis by five inches—guaranteed!” “Boost your sexual performance with this new, all-natural supplement!” With such […]
New Patient Portal Instructions – Tower Urology Los Angeles
Tower Urology is excited to introduce you to our patient portal. On the portal, you can:
Securely communicate with your doctor
View your health information
And even manage your family’s care!
Sign up for an account to access the above and more anytime and anywhere! It’s an easy way to stay connected and communicate with Tower Urology about your healthcare.
To gain access to our new patient portal, please get in touch with Tower Urology at (310) 854-9898
You have the right to receive a “Good Faith Estimate” explaining how much your medical care will cost.
You have the right to receive a Good Faith Estimate for the total expected cost of any non-emergency items or services. This includes related costs like medical tests, examinations, office visits prescription drugs, and equipment (items or services reasonably expected to be furnished by this practice).
Make sure your health care provider gives you a Good Faith Estimate in writing at least one (1) business day before your medical service or item. You can also ask your health care provider, and any other provider you choose, for a Good Faith Estimate before you schedule an item or service.
If you receive a bill that is at least $400 more than your Good Faith Estimate, you can dispute the bill.
Make sure to save a copy or picture of your Good Faith Estimate.
For questions or more information about your right to a Good Faith Estimate, visit https://www.cms.gov/nosurprises. To speak to our billing department, please call (310) 854-9898.
Thank you.
Your friends at the clinic of Tower Urology
Privacy Policy, Website Terms and Conditions of Use
The clinic of Tower Urology (hereafter referred to as the “Clinic”) is dedicated to improving the quality of medical and health information available on the world wide web. As a result, we pledge the following:
Authoritative
Any medical or health advice provided and hosted on this site will only be given by medically trained and qualified professionals unless a clear statement is made that a piece of advice offered is from a non-medically qualified individual or organization.
Complementary
The information provided on this site is designed to support, not replace, the relationship that exists between a patient/site visitor and his/her existing physician.
Privacy
Confidentiality of data relating to individual patients and visitors to a medical/health Web site, including their identity, is respected by this Web site. The Web site owners undertake to honor or exceed the legal requirements of medical/health information privacy that apply in the country and state where the Web site and mirror sites are located.
We use Google Analytics on our website to analyze the audience of the website and improve our content. No personal information is ever collected from Google Analytics. For further information on the privacy policy concerning Google Analytics, please go to: https://support.google.com/analytics/answer/6004245?hl=en.
Attribution
Where appropriate, information contained on this site will be supported by clear references to source data and, where possible, have specific HTML links to that data. The date when a clinical page was last modified will be clearly displayed (e.g. at the bottom of the page).
The source of the medically related content are written by the doctors and medical staff of the Clinic. Authorship is attributed on the content page and all information is medically reviewed by the Clinic’s education team.
Justifiability
Any claims relating to the benefits/performance of a specific treatment, commercial product, or service will be supported by appropriate, balanced evidence in the manner outlined above.
Please note that there are no guarantees that every medical treatment or surgery will satisfactorily cure or repair every condition, for every person, every single time.
Regarding any before and after pictures displayed on our website, the following are true:
The person in the before picture and the after picture are the same.
The pictures were not digitally modified nor in any way enhanced.
Each surgery has unique results for each patient and no one can ever guarantee the same result for every person visiting our website.
The Clinic has the explicit consent of the patients to take their pictures and publish them on your website.
Transparency
The designers of this Website will always seek to provide information in the clearest possible manner and provide contact addresses for visitors who seek further information or support. The Webmaster’s e-mail address is webmaster@towerurology.com.
Financial Disclosure No third-party commercial or non-commercial organizations have ever provided any economic support or services for this website. If that ever changes, it will be identified, including the identities of commercial and non-commercial organizations that have contributed funding, services, or material for the site.
Advertising policy
The Clinic does not accept any advertising from any company or individual and never has. If that ever changes, the source of funding will be stated and a brief description of our advertising policy adopted by the Web site owners will be displayed on the site. If advertising and/or other promotional material will ever be presented to website visitors, it will be in a manner and context that facilitates differentiation between it and the original material created by the institution operating the site.
Additional Web Site Terms and Conditions of Use
Terms
By accessing this website, you are agreeing to be bound by this website’s Terms and Conditions of Use, applicable laws and regulations, and their compliance. If you disagree with any of the stated terms and conditions, you are prohibited from using or accessing this site. The materials contained in this site are secured by relevant copyright and trademark law.
Use License
Permission is allowed to temporarily download one duplicate of the materials (data or programming) on the Clinic’s site for individual and non-business use only. This is just a permit of license and not an exchange of title, and under this permit, you may not:
modify or copy the materials;
use the materials for any commercial use or for any public presentation (business or non-business);
attempt to decompile or rebuild any product or material contained on the Clinic’s site;
remove any copyright or other restrictive documentation from the materials; or
transfer the materials to someone else or even “mirror” the materials on another server.
This permit might consequently be terminated if you disregard any of these confinements and may be ended by the Clinic whenever deemed. After permit termination or when your viewing permit is terminated, you must destroy any downloaded materials in your ownership whether in electronic or printed form.
Disclaimer The materials on the Clinic’s site are given “as is”. The Clinic makes no guarantees, communicated or suggested, and thus renounces and nullifies every single other warranty, including without impediment, inferred guarantees or states of merchantability, fitness for a specific reason, or non-encroachment of licensed property or other infringement of rights. Further, the Clinic does not warrant or make any representations concerning the precision, likely results, or unwavering quality of the utilization of the materials on its Internet site or generally identifying with such materials or on any destinations connected to this website
Constraints In no occasion should the Clinic or its suppliers be subject to any harm (counting, without constraint, harms for loss of information or benefit, or because of business interference) emerging out of the utilization or powerlessness to utilize the materials on the Clinic’s Internet webpage, regardless of the possibility that the Clinic or an approved agent has been told orally or in written of the likelihood of such harm. Since a few purviews don’t permit constraints on inferred guarantees, or impediments of obligation for weighty or coincidental harms, these confinements may not make a difference to you.
Amendments and Errata The materials showing up on the clinic’s site could incorporate typographical or photographic mistakes. The Clinic does not warrant that any of the materials on its site are exact, finished, or current. The Clinic may roll out improvements to the materials contained on its site whenever without notification. The Clinic does not, then again, make any dedication to update the materials.
Links The Clinic has not checked on the majority of the websites or links connected to its website and is not in charge of the substance of any such connected webpage. The incorporation of any connection does not infer support by the Clinic of the site. Utilization of any such connected site is at the user’s own risk.
Site Terms of Use Modifications The Clinic may update these terms of utilization for its website whenever without notification. By utilizing this site you are consenting to be bound by the then-current form of these Terms and Conditions of Use.
Governing Law Any case identifying with the Clinic’s site should be administered by the laws of the country of the United States of America and the General Terms and Conditions applicable to the Use of a Web Site.
Privacy Policy
Your privacy is critical to us. Likewise, we have built up this Policy with the end goal you should see how we gather, utilize, impart, and reveal and make utilization of individual data. The following blueprints our privacy policy.
Before or at the time of collecting personal information, we will identify the purposes for which information is being collected.
We will gather and utilize individual data singularly with the target of satisfying those reasons indicated by us and for other good purposes unless we get the assent of the individual concerned or as required by law.
We will just hold individual data for the length of essential for the satisfaction of those reasons.
We will gather individual data by legal and reasonable means and, where fitting, with the information or assent of the individual concerned.
Personal information ought to be important to the reasons for which it is to be utilized, and, to the degree essential for those reasons, ought to be exact, finished, and updated.
We will protect individual data by security shields against misfortune or burglary, and also against unapproved access, divulgence, duplicating, use, or alteration.
We will promptly provide customers with access to our policies and procedures for the administration of individual data.
We are focused on leading our business as per these standards with a specific end goal to guarantee that the privacy of individual data is secure and maintained.
Open Payments Database Notice
For informational purposes only, a link to the federal Centers for Medicare and Medicaid Services (CMS) Open Payments web page is provided here. The federal Physician Payments Sunshine Act requires that detailed information about payment and other payments of value worth over ten dollars ($10) from manufacturers of drugs, medical devices, and biologics to physicians and teaching hospitals be made available to the public.
The Open Payments database is a federal tool used to search payments made by drug and device companies to physicians and teaching hospitals. It can be found at https://openpaymentsdata.cms.gov.
Review Policy
The clinic of Tower Urology is dedicated to transparently publishing customer feedback and reviews. This policy applies to reviews submitted by patients through first- and third-party review sites monitored on this platform. We reserve the right to remove posts, comments, or reviews that violate our content policies and/or are suspected to be fraudulent.