The pudendal nerve is the main nerve of the perineum — the area between the genitals and the anus. It carries sensation to and from the genitals, urethra, bladder, rectum, and skin of the perineal region, and also controls the sphincter muscles that regulate bladder and bowel function.

What is pudendal nerve irritation?
Pudendal nerve irritation (also called pudendal neuralgia or pudendal nerve entrapment when the nerve is physically compressed) is a condition where the pudendal nerve becomes inflamed, compressed, or damaged, causing chronic pain in the pelvic floor region. It’s sometimes called “cyclist’s syndrome” because prolonged pressure from bicycle seats is a common trigger.
What are the common symptoms of pudendal nerve irritation?
The pain is typically felt in the perineum, genitals, buttocks, or inner thighs, and is often described as burning, stabbing, aching, or electric-shock-like. Characteristic features include pain that is worse when sitting and relieved when standing or lying down, as well as urinary urgency or frequency, pain with sexual activity, and sometimes constipation or rectal discomfort.
What causes pudendal nerve irritation?
Causes include prolonged sitting (especially cycling), childbirth trauma, pelvic surgery, repetitive strain from sports or exercise, falls or direct trauma to the tailbone/pelvis, and nerve compression from surrounding muscles or ligaments (particularly the sacrospinous ligament).
How do we diagnose pudendal nerve irritation?
Diagnosis is largely clinical, based on symptom history and physical exam. A pudendal nerve block (an anesthetic injection near the nerve) can serve as both a diagnostic tool and a treatment. Imaging like MRI may rule out structural causes.
What are the treatment options for pudendal nerve irritation?

Treatment ranges from conservative to interventional. Conservative approaches include activity modification (avoiding prolonged sitting), physical therapy focusing on pelvic floor relaxation, and nerve-calming medications like gabapentin or amitriptyline.
More advanced options include pudendal nerve blocks with corticosteroids, pulsed radiofrequency ablation, and, in cases of true entrapment, surgical decompression.
It’s a condition that’s often underdiagnosed because its symptoms overlap with other pelvic pain conditions, so patients frequently see multiple specialists before receiving an accurate diagnosis.
What symptoms of pudendal nerve irritation overlap with what other pelvic pain conditions?
Pudendal neuralgia is notorious for mimicking several other conditions, which is why the average time to diagnosis can stretch years. Here’s how the symptom overlap breaks down:
Interstitial Cystitis(IC) / Bladder Pain Syndrome
Both cause urinary urgency, urinary frequency, pelvic pressure, and pain that worsens with a full bladder. The key difference is that IC pain is typically centered in the bladder itself, while pudendal pain is more perineal, but patients and even clinicians often can’t distinguish between them without targeted testing.
Chronic Prostatitis / Chronic Pelvic Pain Syndrome (CP/CPPS) in Men
This is one of the most common misdiagnoses. Both conditions cause perineal aching, scrotal or penile pain, painful ejaculation, urinary symptoms, and pain that worsens with sitting. Many men diagnosed with “chronic prostatitis” who don’t respond to antibiotics may actually have pudendal nerve involvement.
Pelvic Floor Dysfunction (PFD)
Overlapping symptoms include perineal pressure, pain with intercourse, urinary and bowel irregularities, and sitting-related discomfort. The relationship is also bidirectional — pudendal nerve irritation can cause pelvic floor muscle tension, and hypertonic pelvic floor muscles can compress the pudendal nerve.
Vulvodynia/ Vestibulodynia in Women
Both cause burning, stinging, or rawness in the vulvar region, pain with intercourse (dyspareunia), and sensitivity to touch. Vulvodynia is sometimes a localized manifestation of pudendal nerve dysfunction rather than a distinct condition.
Levator Ani Syndrome

Both cause chronic dull aching or pressure deep in the pelvis and rectum, often aggravated by sitting. Levator ani syndrome specifically involves spasm of the levator ani muscle, but the nerve irritation and muscle dysfunction frequently coexist.
Coccydynia (Tailbone Pain)
Tailbone pain and pudendal nerve irritation share overlapping symptom territory — sitting-related pain, perineal discomfort, and referred pain into the buttocks. Both can also be triggered by falls or trauma.
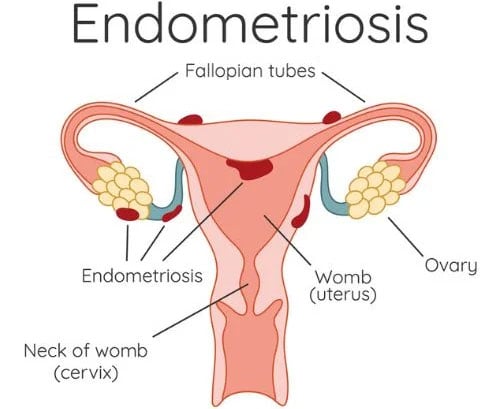
Endometriosis
In women, both can cause deep pelvic pain, painful intercourse, and bowel-related symptoms. Endometriosis is hormonally driven and often cyclical, which helps distinguish it.
However, when both conditions coexist, the symptom picture becomes far more complex, often overlapping and intensifying discomfort. This can make diagnosis challenging and requires specialized evaluation to identify each source of pain and guide appropriate treatment.
Proctodynia / Proctalgia Fugax
Both can cause rectal pain, pressure, and spasm. Pudendal nerve irritation affecting the inferior rectal branch can closely mimic these anorectal pain syndromes.
Both can cause rectal pain, pressure, and spasm. Pudendal nerve irritation affecting the inferior rectal branch can closely mimic these anorectal pain syndromes.
The core diagnostic challenge is that the pudendal nerve supplies such a broad anatomical territory that its irritation can convincingly replicate nearly any pelvic pain condition. A pudendal nerve block that produces significant temporary relief is often the clearest diagnostic signal that the pudendal nerve is the primary driver, which is why it’s such an important diagnostic tool.
Have questions about pudendal nerve irritation? Turn to Tower Urology
Board-certified, fellowship-trained urologists at Tower Urology can help address your concerns about pudendal nerve irritation.
Please make an appointment online or call us at (310) 854-9898.
Tower Urology is a proud affiliate of Cedars-Sinai Medical Center, ranked #1 in California and #2 nationwide by U.S. News & World Report. This partnership reflects our dedication to delivering the highest standard of urologic care alongside the best urologists in Los Angeles. Our years of experience and access to Cedars-Sinai’s world-class facilities ensure that our exceptional and innovative urological care positions Tower Urology as a leader in Southern California.
Tower Urology is conveniently located for patients throughout Southern California and Los Angeles, including Beverly Hills, Santa Monica, West Los Angeles, West Hollywood, Culver City, Hollywood, Venice, Marina del Rey, Burbank, Glendale, and Downtown Los Angeles.